Listen & Subscribe
Listen & Subscribe



Listen & Subscribe

Support Us
Donations will be tax deductible
Subscribe, Review, Listen:



















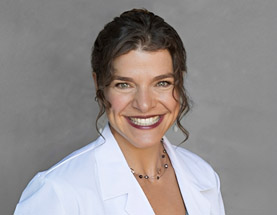
I realized that in medicine…we essentially treat symptoms; we have a sick-care system instead of a healthcare system,” says Elizabeth Parrish, CEO of BioViva. It was her son’s diagnosis and experience receiving treatment for type 1 diabetes that compelled her to learn more about childhood diseases, risks, prevention, experimental medicine, and stem cell regenerative medicine. She explains how effective cell type technologies and regenerative medicine can be at curing a multitude of childhood diseases while at the same time targeting one of the greatest unmet needs: treatment for diseases of biological aging, including cancer, heart disease, organ failure, and Alzheimer’s.
Among the regenerative therapies being explored is polymerase induction, which causes telomere extension for combating diseases of aging while at the same time treating progeria, a childhood disease known to cause “accelerated aging.” Parrish discusses the details of all this and more, including the foundation of BioViva in 2015, her personal experience undergoing two gene therapies, and the global impact that this technology could have on the world.
Learn more about the BioViva mission by visiting https://bioviva-science.com/.
[bg_collapse view=”link” color=”#fff” expand_text=”Podcast Transcript” collapse_text=”Show Less” inline_css=”background:#365969;” ]
Richard Jacobs: Hello this is Richard Jacobs with the future tech and future health podcast. And I have Elizabeth Parish, CEO of BioViva, the company committed to extending healthy lifespans using cell technologies and Elizabeth wears many hats,
Humanitarian entrepreneur, innovator, podcaster and a leading voice for genetic cures, and we’re going to get into why and how. So Elizabeth, thanks for coming.
Elizabeth Parrish: Yeah, thanks for having me on future tech. It’s great to talk to you again.
Richard Jacobs: Yeah! So, you know, it’s okay to have a recap, but what was your whole motivation for wanting to be in the space of medicine and then specifically looking for genetic cures to various problems?
Elizabeth Parrish: All right so what got me started in this area briefly as I can possibly say is my son was diagnosed with type one diabetes after I had done two years of area research in the area of stem cells, so I had been working in the regenerative medicine area trying to figure out that out, what technology was working, whether it was not working, and how to get the education out there so we could get funding through to this viable technology. And when my son was like verifies, notice that there was no translation of regenerative medicine for children with high needs that were in the hospital and there were other kids that were dying of diseases, and I realized that in medicine what we do is we essentially treat symptoms.
We have a sick care system instead of a health care system. We’re not translating, therapeutics through the patients fast enough to save their lives. It appears that bio ethically, we think that patients should rather die than take part in experimental medicine. And I’m really rallied against that 100%. So I went and tried to learn about more uses of regenerative methods medicines specifically in genetics because I had felt for a couple of years working in stem cells that essentially the mechanisms of the epigenetics and the cells, that the genes themselves were responsible for the regeneration. And that if we could have that sort of outcome in a patient’s body without having to apply to stem cells, we would have a much better outcome. So I started looking at genetics, ran into a conference, operating group, met with a bunch of geneticists and specialists in the area, ask them how this technology of aging could be translated to childhood disease because that was my focus to target to cure.
And it turns out that regenerative medicine and the aspects of using gene and cell therapies still stem cells as well will actually create a lot of cures for a lot of childhood diseases. While we tackled the biggest unmet need, which is biological aging, by treating biological aging, we change the outcome of diseases that are preventable like Alzheimer’s, cancer, heart disease, organ failure, like kidney disease, and essentially not bring those cures back to kids and then create a life for kids where they don’t just get healthy for a couple of decades only to become sick. And again, with the diseases that we vastly die of. So that is it in a nutshell and I hope that made sense.
Richard Jacobs: Yeah, well what I wanted to ask you is this many conditions out there and then there are mechanisms. So maybe first, what are the particular conditions that you want to address first? Because you know, no one can really do them all. So is it type one diabetes in children or what is it?
Elizabeth Parrish: So, essentially, type one diabetes is an autoimmune disease. There are a couple of really great, uh, cell type technologies where they take the Beta cells from the patients and put them into the liver or put them into capsules that the immune system cannot target. The cure for it though will vastly be in effecting genetics. We’re not there yet, it’s called a complex disorder, where we’re treating the complex disorder is more on the lines of treating aging with regenerative type therapies, which these kids will need as well. So when we look at biological aging, we’re looking at the hallmarks of aging and you’re right, not one treatment is going to treat the hallmarks of aging. So where we have a platform as called integrative health systems that essentially gives people access to a myriad of different types of regenerative gene therapies that they can participate in to help find the gene therapies that work in certain aspects of the hallmarks of aging and then work those back into treating a multi-cam editorial gene therapy that will treat a disease.
But each one of the gene therapies, we look at Theresa childhood disease. So if you’re wondering where these would work so when you’re looking at regenerative therapy, we’re talking about creating one treatment that affects all of the diseases of aging. And each one of the treatments we look at actually also has an effect of treating a childhood disease. So if you’re, one of the gene therapies we look at is telomerase inductions. So the telomeres are the caps at the ends of your chromosomes and they shorten with each cellular division. One of the treatments for aging will have to be dealing with this problem of cellular senescence and cell proliferation. So you need long telomeres or else this the cell stop dividing. So that treats biological aging, that if we can keep the kilometers long, will very likely, keep a healthier epigenetic state in the cell and avoid things like cancers and other diseases like cardiovascular disease and Alzheimer’s that are associated with short telomeres.
But we can also treat a childhood disease called Progeria. That is the hallmark of that disease is the attrition of Telomeres these kids die in their teens very young. Of all of the same diseases that we die of at much older ages. So it’s considered accelerated aging. Another gene therapy we look at is one that increases muscle mass, and clinical trials about eight out of 10 patients have their muscle mass increased in muscular dystrophy states. We’re using it for an aging population, but you can see how driving the costs down by treating one of the biggest unmet needs the whole population with something like a muscle enhancer, therefore, keeping their body strong and making it so they don’t die from falls associated with frailty, which I just said at the bedside of someone who died that way last week.
By treating the biggest unmet need, we create really affordable therapies that can also treat muscular disorders, myopathies, and young children. And it just goes on one after another with the gene therapies that we’re looking at right now, whether we’re looking at four different gene therapies we will expand that as we go. George Church, one of our scientific advisors is a professor of genetics at Harvard, just came out with his list of 45 genes associated with treating aging, and some of them we will actually pull and start looking at for specificity as well. But all of them that we target will also treat childhood diseases as well.
Richard Jacobs: Yeah, I would think just visually, you know, if you want to study aging, we’ll get old people, my children that I know that you want to hold Chubb children because you know, that population is near and dear to your heart and many people’s hearts. Obviously, they either have or don’t have children. Do you think that in terms of this study of aging and had slow aging or reverse it or stop it, where is the most useful information? Is it in studying children or is it in studying old people or what, what do you think the best learnings will come from?
Elizabeth Parrish: There so that the best learning will come from the biggest cohort and that will be aging adults, this is the biggest, fastest way to get there as far as you agree right now. It’s in the Meta-analysis of research that has already happened. That’s where you would have to go to, right now what we’re doing is we’re starting to get the first human data on how these gene therapies perform in humans because it’s, you know, one human outweighs a thousand-mile mass studies and too, it just becomes exponentially more relevant.
And so right now the platform company that we work with, integrative health systems, which we hope will become an accepted tested system for biotechnology in general. We hope it’s the first place investors take companies that they’re interested in, that they think are ready for human studies to find out how drugs work in humans before they start to raise $1 billion for the regulatory service. That system right now for us preparing to handle the data, but they already have many patients who have taken regenerative gene therapies and then via the bioinformatics platform of BioViva is going to be handling that data and assessing, how these patients are doing, how the drugs are performing the safety and trying to glean some amount of efficacy and low numbers as those numbers grow. I am no longer the only patient with dual gene therapy. There are several patients now that through that platform who has taken that and we’re really excited about handling their data.
Richard Jacobs: Okay! You’ve had dual gene therapy. What have you had done to yourself and what were the effects that you noticed?
Elizabeth Parrish: Oh right! So yeah, we should probably for listeners go back a little bit so when I started BioViva I started it in 2015 and the whole idea of BioViva was to get data on how well these drugs performed, so stepping forward as the CEO of the company I took the first two gene therapies to treat biological aging one of them was the Myostatin inhibitor the gene therapy that increases muscle mass in Douchey and muscular dystrophy. So I was not the first to use that, but I was the first that concept for aging for the company. And the second one was the telomerase inducer, which had not been used in Vivo, meaning an antibody and a human. It had been used in human sound.
It had been used for over a decade in animal studies. It had reversed biological aging and gene knockout mice and it had lengthened the healthy life span of aged mice. So we were really excited about that. We’re now doing another study for in BioViva, for telomerase induction in mice with our new viral vector deliveries, and we’ll be doing a longevity study. Now, the mice just showed up to the university and they’re going through their quarantine now and we’re about to start. So, we’re also doing separate tests, for the Myostatin inhibitor in those mice as a longevity study as well. So we’re doing a new delivery.
Richard Jacobs: So what is the Myostatin inhibitor? And what does that telomerase inductor, what are those things?
Elizabeth Parrish: Yeah, so a Myostatin inhibitor so that’s a really good question. And especially we don’t have visuals when people are just listening. I’m going to try to make this as at Licit as possible. A lot of people just tune out. They’re like, what is that? Like? Just stop. I don’t even know what words you just said. So Myostatin is a protein in your blood that regulates muscle growth. So when you’re young and you have a lot of growth hormone, it keeps your body from expending a bunch of energy, creating huge muscles that might not be great for your metabolic state. Meaning maybe you don’t have enough nutrition for all these muscles. So it’s a regulator to muscle growth, as you age, that regulator, it becomes counterproductive. We start to lose muscle mass at percentages after the age of 30, 35, depending on the person and it becomes detrimental. Frailty is a real issue with the aging falls, broken hats, not being able to climb stairs, walkers, you’ve seen that that’s called palliative care.
When we start throwing devices at people because they don’t have the strength anymore to hold themselves up, that’s called Sarcopenia. There’s another condition called Pic Haq Fia, that happens after cancer treatments and it’s also muscle wasting associated with chemotherapy. So muscle wasting happens and because of bio Stanton in your blood inhibiting muscle growth, it becomes detrimental. So Myostatin inhibitor, you can imagine inhibitor means to stop something. It actually blocks Myostatin’s action of performance, not 100%. That’s why with the gene therapy, we don’t see people looking like the incredible hulk. But what happens is we titrate, meaning we decide the amount of dose that a person needs to take to gain muscle mass in Myostatin inhibitor. In the case of gene therapy is a gene that creates a protein that you can imagine going out in the blood. It finds the Myostatin and it finds it so that it cannot regulate your muscle growth anymore in the way that it did. And again, we don’t incredible use bodies from doing this. We get 10, 20% muscle mass gain from the type of therapeutic doses that are given. And so that’s what that is. Did that make sense?
Richard Jacobs: Yeah, it makes sense. Why did you have this therapy done? Were you experiencing muscle wasting and when you ripped afterward? So, you know, what did you experience?
Elizabeth Parrish: So what sort of outcome would you get from that? So when I did it because I was my forties when I did the gene therapy, I was a 44 and what happened it is what we expect to see happened. Actually, I had been exercising a lot before I did the gene therapy and after I did the gene therapy I was on some immune suppression. So I wasn’t doing a lot of exercises. And then it just so turns out that the information was leaked out of the company that we had treated the first patient. And at that point I was on a lot of airplanes, not exercising regularly and still, we found muscle mass increase. We not only saw that we do MRI images before and after we saw a decrease in white fats, which we would expect with muscle mass increase the fat between the muscles also decreased. We saw an increase in insulin sensitivity. So the reason that you would do a gene therapy like this is not just for muscle mass loss, it’s also for what we call metabolic disorder or things that lead to type two diabetes that is aging-associated. So when you increase muscle mass, you increase insulin sensitivity and you decrease white fat and we believe that that will be great protection for type two diabetes. I did not have type two diabetes and I did not have clinical sarcopenia. I simply think that an aging body needs to be treated as soon as possible before you’re diagnosed with those diseases or soon after if you can be. We also are looking to treat vastly super-aging people, we’re putting up a campaign its called help them see the future through maximum life foundation. And we are very interested in treating a very old population, but I believed that these gene therapies will be worked back as preventative medicine as a future of patients rather than using them before they get sick. rather than waiting to get sick.
Richard Jacobs: When you did the last Myostatin inhibitor you experienced a lot of benefits, you said you had to have your immune system suppressed. Why is that?
Elizabeth Parrish: So for a gene therapy you temporarily have your immune system suppressed around the gene Caribbean for the few weeks after the gene therapy. You come off of the immune suppression slowly. Now, the reason that you do that is so the uptake of gene therapy is the best possible. You don’t want to have a reaction to gene therapy. You want to give the gene therapy time to work. You don’t want your immune system scan emerging out of the therapeutic. And so it’s not a huge immune suppression at all. It’s a light immune suppression, but it does affect your immune system. It has effects on you that you probably won’t be doing a lot of exercising during that time. You’re trying to lay low, you’re not exposing yourself to a lot of contaminants and so it definitely disrupted regular, exercise pattern for a few weeks.
Richard Jacobs: But it’s no different than I guess if you were on chemo, you know, from what I’ve heard, the patients have to do the same thing.
Elizabeth Parrish: If you’re on chemo that’s much more serious than if you are immune suppression. It’s a little bit more like you if you’re somebody who had a severe allergy and you went to the doctor and you would take a week, two-week-long treatment of immune suppression that’s not something that would actually make you deathly ill if you are exposed to some minor infection. So yeah, it’s nothing that severe. I should probably make that clear and I’m not trying to be appealing to people at all. I’m just telling you the truth. It is not going to be a severe process to go through gene therapy.
Richard Jacobs: Oh, that’s good.
Elizabeth Parrish: I think I still need to explain the telomerase inducer. Do you want me to do that?
Richard Jacobs: I was just about to ask you about telomerase inducer. So what, what was the reason for that? What did it do to you etc.? Tell me about that.
Elizabeth Parrish: Well short telomeres are correlated with all of the diseases of aging. They’re associated with some childhood diseases as well. We know that critically short telomeres are generally always found around the point of diagnosis. We know that telomere length is associated with healthy cell division and so even if you could discount everything else, you cannot discount short telomeres and cell division cell stops dividing when two get short. And one of the things that are a problem and a regeneration of the body is stem cell depletion.
We want stem cells not to get depleted and therefore lengthening kilometers give them healthier divisions themselves. So this is a technology that’s very exciting. It’s a technology that’s been around for decades. It had been speculated, postulated when researchers argue about it, and yet there was no human data. So there’s really nothing to argue about whether it works or doesn’t work is completely irrelevant until you get human data, and I’m always surprised as people being in these long debates as to whether a technology works or not when it hadn’t been applied. And so I took that technology to lengthen the telomeres vastly targeting the stem cell populations and dividing cells. Telomere attrition is one of the hallmarks of aging, so it’s something that needs to be addressed. It is when you lengthen telomeres, it just amazingly targets a bunch of other hallmarks of aging and we can talk about them.
So why would you want to live with healthy cell division, you want useful cells and it does seem to change the profile of the cells. So it may have got the epigenetic effects on the cells creating a more useful cell, so it definitely helps revitalize Monica Mitochondria. Mitochondrial dysfunction is being numbered one homework of aging that we see across every disease of aging. It also helps with some cell communication issues and it may in fact help with stem cell depletion. And that would be one of our major targets is make sure that your body doesn’t deplete of stem cells, which are your regenerative cells that can differentiate into any type of cells that are needed to repopulate an area of your body when there’s damage so that sort of regeneration is something that we definitely want to target.
And so that is why I took the gene therapy to lengthen telomeres and to be very clear, the gene therapy is the only known way and assured way to length telomeres right now. I’m saying that there are different genetic ways to lengthen telomeres all of them have to effect the telomerase gene thereby lengthening the telomeres. And I’m basically bouncing this against small molecules so there is no known small molecule that I have ever seen that has research that really reflects that you can lengthen telomeres in any other way. And I’m not a proponent for small molecules because if you have a small molecule that’s turning on the H reck gene is very likely turning on other genes as well. So I think that this gene therapy is the most targeted best way of actually stimulating telomerase and like putting tumors.
Richard Jacobs: How do you lay hands? Is there a gene you’re turning on?
Elizabeth Parrish: Yeah. It’s called the H-tert gene. And what it does is it codes for a protein called telomerase. And the tall telomerase is actually what the chromosome uses to rebuild the telomere at the end of the chromosome. That’s a great question.
I know that age term is the gene that means a human, telomerase, a producing gene. The telomerase is the protein that the gene makes, genes code for proteins and proteins make you so it codes for gene for a protein called telomerase. And that telomerase which is the cap at the end of the chromosome.
Richard Jacobs: What did you experience was to stretch them out?
Elizabeth Parrish: Right, so when we did testing, we saw telomere lengthening and with white blood cells. So that’s the traditional test. That’s the most common test out there. And so we use the traditional third-party testing and we continue to test those. We can assume that we targeted a lot of the cells in my body, but not all of that because gene therapy doesn’t have right today, the ability to target 100% of the cells, but the outcome that we saw that we think that is associated with the telomerase induction is, of course, the language millimeters and the T lymphocytes. I had a reduction in inflammation and by the body that was significant after the therapy, it was about a six-fold decrease from the inflammatory markers before and I also saw a reduction and triglyceride levels of about 50%. So we would think we would consider that as correlating with better heart health.
Richard Jacobs: Yeah, that’s far more than any cholesterol-lowering drug.
Elizabeth Parrish: Yeah! Right, and actually doing it a healthy way. So what we’re hoping with gene therapy is honestly if we see the same outcome from 10 patients that we saw in the body that would be hands down the most powerful drug on the planet. Plus it would be essentially natural. So it basically hits the aesthetics of what people really like. So instead of taking a small molecule that might damage your liver or hurt your kidneys and have some off-target effect of maybe lowering some cholesterol levels, but putting you at higher risk for type two diabetes and dementia, we’d be talking about just at the cellular level upregulating a gene that already exists in your body. It’s creating a targeted therapeutic protein with no known negative effects. It’s pretty powerful.
Richard Jacobs: You said these gene therapies, do they need to act locally or systemically as fine? I mean, what governs whether something used to act locally or systemically in Canid? Do you know how difficult it is that a problem?
Elizabeth Parrish: That is a great question and that is why I mentioned how many cells we can target with telomerase. And that’s why I didn’t mention cell targeting issues with the Myostatin. So with the telomerase inducing gene therapy, the problem is telomerase has a localized effect, meaning it’s not really shared outside of the cell and it only has an effect on the cells that are transfected with the gene therapy or transduced in the case of the body. So if the gene gets into the cell that has a beneficial effect on that cell, but it doesn’t have one systemically.
That’s why with the age gene therapies tend to be very expensive because they’re created in titrations and are trying to target as many cells in the body as possible. The Myostatin inhibitor, on the other hand, is the system that has a systemic delivery, so it’s made, if we targeted the cells the protein is made in those cells, but it’s shared out into the bloodstream. So it has a full-body effect. Although if you do the Myostatin inhibitor and you have it, let’s say you had it directly injected to certain muscles, those specific muscles will benefit the most and then it will have a system systemic effect on the rest of the body. But so you know, you do want to think about targeting if a person has particular atrophy in a certain area, you’re going to have a better response, right where you put it. The gene itself is the new thinking and the new therapies that are coming out that are more systemically given targeting muscle skeletal muscles with certain tropism. So certain a vector delivery that is specific to musculoskeletal delivery.
Richard Jacobs: So what’s the particular role of BioViva? I mean, there’s so much to do, can’t one person can’t do it all no matter how much Myostatin is inhibited. So what’s the role of BioViva?
Elizabeth Parrish: We’re a bioinformatics company, so we think that the most important thing is gathering data on what works and then getting those therapeutics that actually work in studies into the regulatory system as fast as possible using the study data as the impetus for accelerating trials in certain areas. The trial, the regulatory area has a 94% cellular rate of drugs. So even if you know your drug is going to work but you pick the wrong endpoint, you will fell. So our study partner actually gives us the ability to look at data, know where it works and put it together in the therapy. But we also have a research arm. So our research and development arm at university is for a new vector that can actually carry instead of today’s most common vector, which can barely carry one gene in a promoter, it can only carry a very small package. Our new vector delivery could carry at least five to 10 times that much. So on the research and development side, what we want to do is we want their things or gene therapies available in the next 10 years because this is the slow development of research and development. And one of them is for non-systemic delivered proteins. So one would be a gene therapy where you have to target most cells in the body and we would package the gene of choice, many genes of choice into that therapy. And the second delivery would be a systemically delivered a protein. So it would be okay. You would in fact use a lower dose because you would have a systemic outcome from the therapeutic.
So on the research and development side, we are working on the delivery method for gene therapy. That’s one of the reasons why all of the states is important and why we’d want to look at so many different genes and that on our site, we’re just doing the bioinformatics, looking at biological aging in November, we should have a repository system online that people can use and bring their multi-domain data.
We’re hoping to also encourage biohackers to come and put their pre and post data so that you know, you’re active. Biohacking is not a selfish act. It goes farther than yourself to help a lot of other people and then what we’re doing most importantly there is we are handling our partner’s patient data in order to analyze how well those gene therapies work. So we can answer to the regulatory system on addressing these advances forward show where they work, where they don’t work, no data are hidden and advancing therapeutics for new rooms. Again, in these more mainstream areas where we might be able to by treating such a large unmet need actually create affordable drugs.
Richard Jacobs: What are some of the other therapies, the names, and maybe act that’s gene therapies that are here perhaps you’re in clinical trials, are they very close to, they’re showing considerable promise in addition to, it’s a laborious induction and addition to Myostatin inhibitors.
Elizabeth Parrish: Well so other genes that we’re looking at is we’re looking at PGC one Alpha for obesity to treat obesity. And we’re looking at closer to treat cardiovascular disease and chronic kidney disease with the hopeful outcome and increase cognition also close as seems protective against all-timers. So that’s things that we’re looking at in the traditional regulatory system right now. There are four past gene therapies all of them coming with an absurd excruciating price that most people can’t afford and we’ve radically needed to change that. And that’s one of the problems of looking at orphan diseases, that don’t have a large population is payers want to recoup the money that they’ve spent on research and development and getting a drug to market. And it just turns out to be a very inhumane okay. The outcome as far as the cost associated with those gene therapies they’re considered a onetime treatment procure.
So people should know that about gene therapy, this is the benefit. This is essentially the future of getting you off of trying to take a pill every day. Things that were not very good at, I’m trying to get an injection every three months or whatever your therapeutic dose looks like, a gene therapy gives you the ability to a lifetime therapy. Even those companies that are not sure that they know that their therapy will last light’s lifetime, but they’re hoping for 10, at least 20 years, maybe a lifetime, and this is the power of the technology. And I think that putting a highly high price tag on that and he’s just going to shut people out from the humane use of treating disease. Plus when you’re creating something like biological aging, I mean, seriously the whole population of the earth, the whole planet right now that World Health Organization said that no communicable diseases which are vast that diseases of aging kill 70% of the global population by 2050, it’s estimated that aging will be the biggest killer in every country of the world.
And this doesn’t need a high price tag for those companies to benefit from selling technology. This is something that we need to get out of cost affordably to patients when the technology is predictable. That’ll take some amount of years but it is a huge savings two countries, you know, each one of the agent diseases about a trillion-dollar cost. And then if you think about sharing these childhood diseases, which is my focus on the top of that you’re looking at an extraordinary amount of savings to insurance companies, providers, governments, society at large. There’s a lot of money lost people and the benefits are immersed. The benefits can be shared globally rather than to very few companies.
Richard Jacobs: Very good! So what’s the best way, well, before that, what are some milestones that you’re going to be looking to hit in the next year or two or three years?
Elizabeth Parrish: Oh, yeah. Well, you know, right now we’re just diligently working on a HIPAA compliant, uh, GDPR compliant bioinformatics sites so that we can handle all of this data. We’re working towards patient safety. We’re huge advocates on our slide to making sure that everything, the call site is running as smoothly as possible, but they are very professional. They know what they’re doing, but you know, where we’re constantly making sure that safeguards are put in place. We are working on, so that, you know, this year we hope to see a hundred patients. Next year we hope to see a thousand patients come through the integrated health system, a platform so we can analyze the data on these therapeutic interventions.
And we hope that to exponentially shoot up year by year. I got on the bioinformatics side, we have, and we’re working with a couple of groups building the front end and the back end of a very secure site for patient data. That’s a big benchmark to get over and in the research and development, we will be waiting for the first outcome of these studies over the next eight to 10, 10 months plus a, we’ll be building new constructs that will be tested of multigene delivery with the same factor. So we’ve got, we’re really busy right now. We are really busy and every one of the aspects of this company. So there’s a tremendous amount going on.
Richard Jacobs: Well very good, what’s the best way for people to find out more perhaps you read papers or suppressed releases in context?
Elizabeth Parrish: Right? So if you want to learn more about BioViva, go to bioviva-clients.com you can learn about what we’re doing there. We’re really sorry about the state of the website. If you know a website developer that’s really good, please contact me. So we had a couple of not that great experiences, so forget the site but enjoy the information. And if you want to learn more about treating aging, Go and read research papers or hire a researcher. Ever read research papers. You’re going to be so thrilled. Really do the diligence and then you’ll know why we’re so excited otherwise you’re gonna end up in a debate with someone and they’re going to go, oh, I don’t think that’ll work. And then you’re really just like bringing it down to opinions. Look at the damn. Science is really good.
Richard Jacobs: Well very good. Well, thanks for coming back, and again I don’t envy the amount of work you’re going to do for an excellent cause, so thank you so much for what you do and for being here.
Elizabeth Parrish: Yeah! Thank you. It’s, it’s my passion. It’s my life. I’d rather work than do anything else. I am at your service. I am your servants, please, you know to keep us accountable, ask us questions, keep us diligent and be excited about the future and want to people want to volunteer and participate. You know, please reach out to us where we’re always looking for an extra hand and extra help.
Richard Jacobs: Thanks for coming.
Elizabeth Parrish: Yup! Thanks for having me.
[/bg_collapse]
Podcast: Play in new window | Download | Embed
Subscribe, Review, Listen:










SHARE THIS PODCAST




Support Us:
Donations will be tax deductible
Subscribe, Review, Listen:

Support Us:
Donations will be tax deductible
Subscribe, Review, Listen:

Support Us:
Donations will be tax deductible
Subscribe, Review, Listen:

Support Us:
Donations will be tax deductible
Subscribe, Review, Listen:
Support Us:
Donations will be tax deductible
Subscribe, Review, Listen:
















Subscribe to Our Newsletter
Get The Latest Finding Genius Podcast News Delivered To Your Inbox